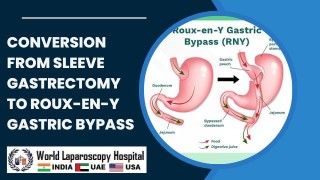
Video of sleeve gastrectomy in a patient previously operated on for ventral hernia
Add to
Share
521 views
Report
8 months ago
Description
Generally, having a sleeve after incisional hernia repair, even with mesh, shouldn't be a problem. If you go through Palmer's point, you don't have to worry about the mesh lingering in the abdomen. All laparoscopic incisions are small and don't disrupt the integrity of the mesh. The only incision that's slightly larger is the one where the resident is removed through the abdomen. Ideally, you want to perform the sleeve laparoscopically. Yes, there will be a lot of adhesions, but an experienced laparoscopic bariatric surgeon can perform it with a laparoscope. The mesh can be re-sewn and will heal. It's difficult to know without knowing where the mesh was placed on your abdominal wall, but I've operated on many patients before for hernia repair, and it's not an insurmountable challenge. If the hernia was from a prior C-section, meaning it's low on your abdominal wall, the laparoscopic port sites for VSG shouldn't interfere. The association between intra-abdominal pressure and subsequent abdominal wall hernias, among other symptoms, is a serious chronic condition. The optimal management of these manifestations is still controversial. The aim of this study was to assess the early postoperative outcomes of the surgical approach of laparoscopic ventral hernia repair (LVHR) with sleeve gastrectomy in morbidly obese patients. This is considered one of the most common risk factors for the development of anterior abdominal wall hernias.1 This may be explained by the increased intra-abdominal pressure and reduced compliance of the abdominal wall associated with obesity. Furthermore, obesity is associated with impaired wound healing.2 The increased risk of developing incisional and recurrent hernias is reflected in the consistently increased incidence of such hernias in obese patients.3, 4, 5, 6 Due to the progressive nature of obesity, the rate of abdominal wall hernia repair in these patients increases proportionally. However, it remains challenging to determine the optimal timing and type of ventral hernia repair given the high recurrence rates. Therefore, surgical management of obesity is a valid option in these patients. Ventral hernia repair is one of the most frequently performed interventions in general surgery, including repairs of both incisional and recurrent types.8 Several techniques have been described for both open and laparoscopic approaches without a significant difference in recurrence rates. However, the laparoscopic approach has advantages in fewer wound-related complications, faster recovery, and improved quality of life.9 10 11 Several studies have considered laparoscopic ventral hernia repair (LVHR) with intraperitoneal mesh (IPOM) as the gold standard.1 Currently, the best approach in managing patients who are candidates for weight loss or metabolic surgery and who have anterior abdominal wall hernias is still a subject of debate due to the lack of an evidence-base for consensus. The main controversy is whether to perform mesh repair in a clean-contaminated area with the risk of infection or an anatomical mesh-free repair with a known higher rate of recurrence. At the same time, the postoperative risk of hernia strangulation or strangulation is a concern if it is left unrepaired.
Similar Videos