Hysteroscopic Submucous Myomectomy
Add to
Share
1,570 views
Report
9 months ago
Description
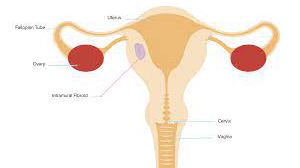
Submucous fibroids (also called submucosal myomas) are benign smooth muscle tumors of the uterus that grow just beneath the endometrium and protrude into the uterine cavity. These fibroids are commonly associated with heavy menstrual bleeding, infertility, and recurrent pregnancy loss. Hysteroscopic submucous myomectomy is considered the gold standard minimally invasive procedure for the removal of submucous fibroids, as it allows direct visualization and precise resection without abdominal incisions. Indications Hysteroscopic myomectomy is typically recommended in the following cases: Abnormal uterine bleeding (menorrhagia, metrorrhagia, or prolonged periods). Infertility or recurrent miscarriage associated with distortion of the uterine cavity. Anemia secondary to excessive menstrual blood loss. Failed medical management of symptomatic fibroids. Submucous fibroids classified as FIGO types 0, 1, and selected type 2, depending on size and accessibility. Preoperative Evaluation Ultrasound (Transvaginal / Saline Infusion Sonography): To assess number, size, and location of fibroids. Hysteroscopy: Direct visualization of the uterine cavity. MRI (in select cases): For mapping fibroid extent, particularly for larger or multiple myomas. Blood workup: Hemoglobin levels, coagulation profile, and fitness for anesthesia. Technique of Hysteroscopic Submucous Myomectomy Anesthesia: The procedure is usually done under general or regional anesthesia. Cervical Dilatation: The cervix is dilated to allow insertion of the hysteroscope. Distension Medium: Normal saline or glycine is used to expand the uterine cavity for clear visualization. Visualization: The hysteroscope is introduced into the uterine cavity, and the fibroid is identified. Resection: Resectoscope with monopolar/bipolar loop is used to shave off fibroid tissue in small fragments. Alternatively, mechanical morcellators or hysteroscopic tissue removal systems may be used. Completion: Once fibroid tissue is completely removed and the cavity restored, fragments are evacuated. Hemostasis: Achieved with electrocautery or natural contraction of the uterus. Postoperative Care Most patients are discharged the same day. Mild cramping or spotting may occur for a few days. Analgesics and prophylactic antibiotics may be given. Avoid intercourse and tampon use for 1–2 weeks. Follow-up hysteroscopy may be scheduled in selected cases, especially when fibroid size was large or incomplete resection was anticipated. Advantages of Hysteroscopic Myomectomy Minimally invasive (no abdominal incision). Daycare procedure with quick recovery. Fertility-preserving surgery. Effective in controlling abnormal uterine bleeding. Low complication rate when performed by experienced surgeons. Potential Complications Although rare, complications may include: Uterine perforation. Excessive bleeding. Fluid overload (from absorption of distension medium). Intrauterine adhesions (Asherman’s syndrome). Infection. Outcomes and Prognosis Symptom relief: More than 80–90% of women report significant improvement in bleeding. Fertility outcomes: Studies show improved pregnancy rates after removal of submucous fibroids, particularly in women undergoing assisted reproductive techniques. Recurrence: New fibroids may develop, but recurrence at the same site is uncommon if resection is complete. Conclusion Hysteroscopic submucous myomectomy is a safe, effective, and fertility-preserving surgical option for women suffering from symptomatic submucous fibroids. With advancements in hysteroscopic instruments and energy sources, this technique has become the first-line approach for managing intrauterine fibroids, offering rapid recovery, minimal morbidity, and excellent clinical outcomes.
Similar Videos